
SYB
SYB
Place
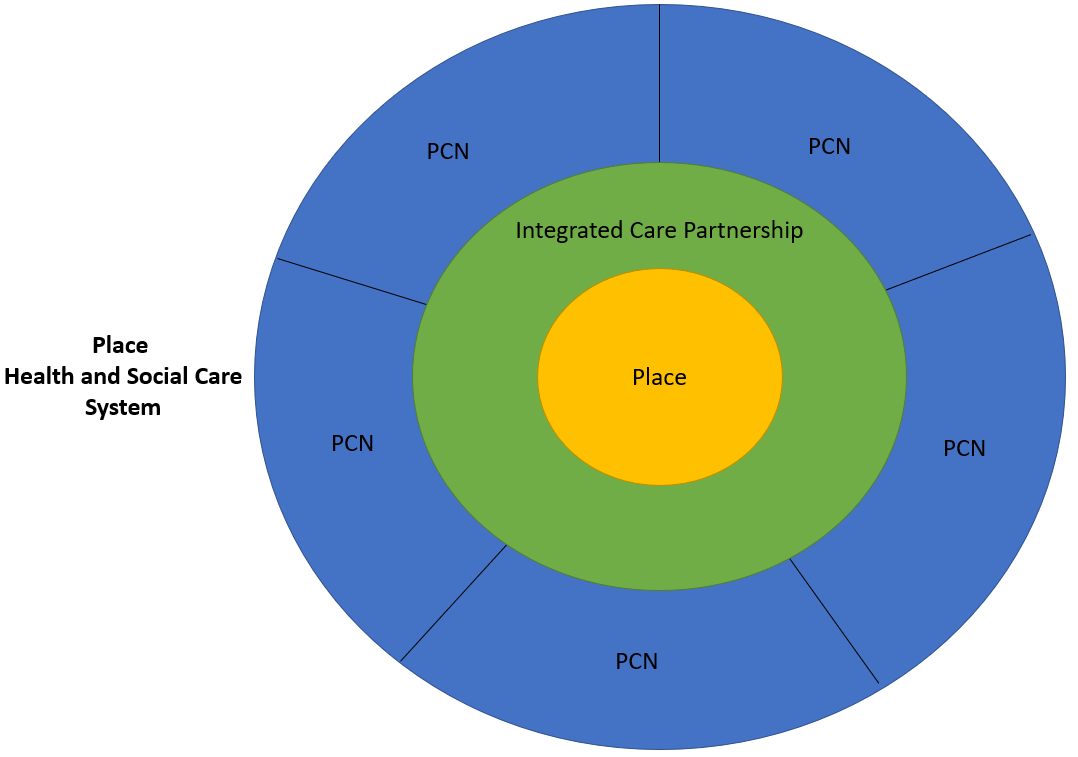
Integrated care Partnership
Membership
Not prescriptive – depends upon local needs
- Local government
- NHS
- Health and Wellbeing boards
- Social care
- Voluntary, community, and social enterprise sector
- Employers
- Housing
- Education
- Criminal justice
Core purpose
• improve outcomes in population health and healthcare
• tackle inequalities in outcomes, experience, and access
• enhance productivity and value for money
• help the NHS support broader social and economic development.
Principles
- Come together under a distributed leadership model and commit to working together equally.
- Use a collective model of decision–making that seeks to find consensus between system partners and make decisions based on unanimity as the norm, including working though difficult issues where appropriate.
- Operate a collective model of accountability, where partners hold each other mutually accountable for their shared and individual organisational contributions to shared objectives.
- Agree arrangements for transparency and local accountability, including meeting in public with minutes and papers available online.
- Focus on improving outcomes for people, including improved health and wellbeing, supporting peopleto live more independent lives, and reduced health inequalities.
- Champion co–production and inclusiveness throughout the ICS.
- Support the triple aim (better health for everyone, better care for all and efficient use of NHS resources), the legal duties on statutory bodies to co–operate and the principle of subsidiarity (that decision–making should happen at the most local appropriate level).
- Ensure place–based partnership arrangements are respected and supported, and have appropriate resource, capacity and autonomy to address community priorities, in line with the principle of subsidiarity.
- Draw on the experience and expertise of professional, clinical, political and community leaders and promote strong clinical and professional system leadership.
- Create a learning system, sharing evidence and insight across and beyond the ICS, crossing organisational and professional boundaries.
Integrated Care Board
Membership
- Board (minimum requirements)
- Chair
- Independent non executive directors x 2
- Chief executive
- Director of finance
- Director of nursing
- Medical director
- Partner members
- Trusts (hospital and community)
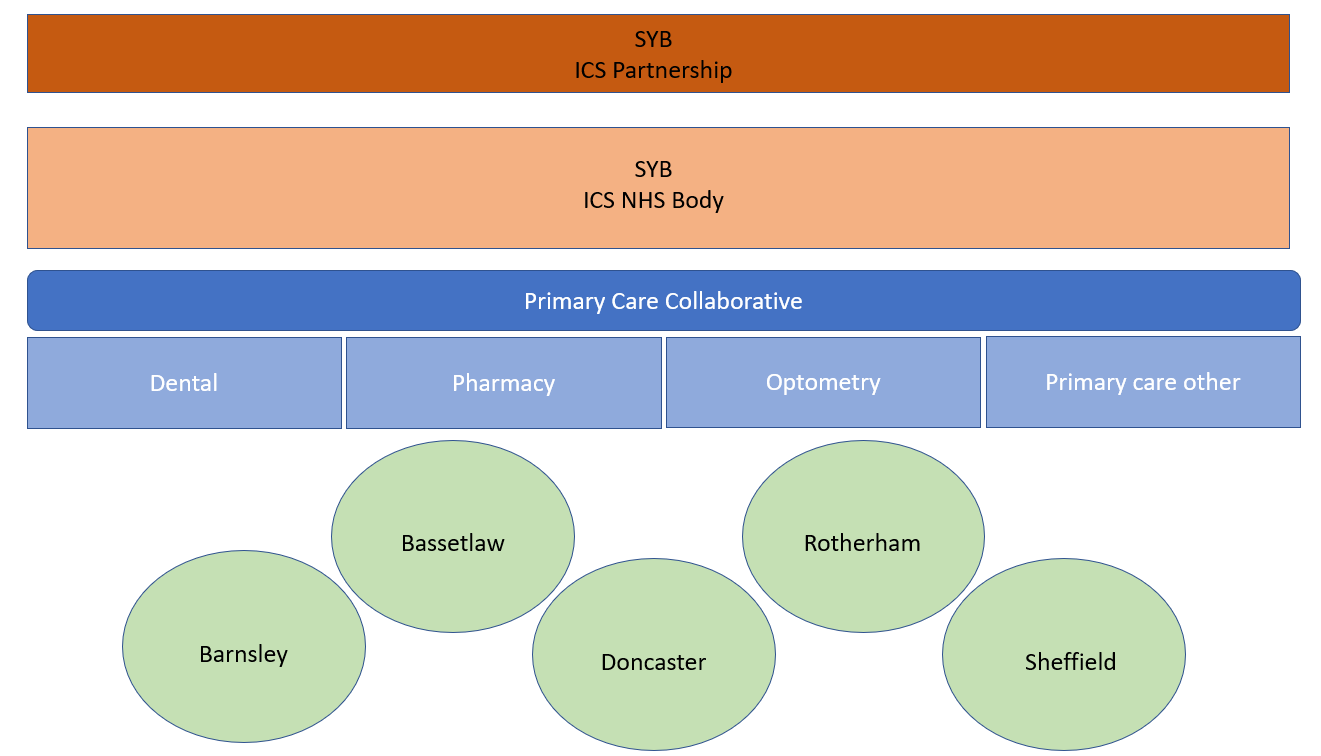
- Primary care (medical, pharmacy, dental, optics)
- Local authority
Core purpose
• improve outcomes in population health and healthcare
• tackle inequalities in outcomes, experience, and access
• enhance productivity and value for money
• help the NHS support broader social and economic development.
Functions
- Developing a plan to meet the health needs of the population within their area, having regard to the Partnership’s strategy.
- Allocating resources to deliver the plan across the system, including determining what resources should be available to meet the needs of the population in each place and setting principles for how they should be allocated across services and providers.
- Establishing joint working arrangements with partners that embed collaboration as the basis for delivery of joint priorities within the plan. The ICS NHS body may choose to commission jointly with local authorities.
- Establishing governance arrangements to support collective accountability between partner organisations for whole–system delivery and performance, underpinned by the statutory and contractual accountabilities of individual organisations, to ensure the plan is implemented effectively within a system financial envelope set by NHSEnglandand NHS Improvement.
- Arranging for the provision of health services in line with the allocated resources across the ICS through a range of activities
- Leading system implementation of the People Plan by aligning partners across each ICS to develop and support the ‘one workforce’, including through closer collaboration across the health and care sector, and with local government, the voluntary and community sector and volunteers
- Leading system–wide action on data and digital
- Using joined–up data and digital capabilities to understand local priorities, track delivery of plans, monitor and address variation and drive continuous improvement in performance and outcomes.
- Working alongside councils to invest in local community organisations and infrastructure and, through joint working between health, social care and other partners including police, education, housing, safeguarding partnerships, employment and welfare services, ensuring that the NHS plays a full part in social and economic development and environmental sustainability.
- Driving joint work on estates, procurement, supply chain and commercial strategies to maximise value for money across the system and support these wider goals of development and sustainability.
- Planning for, responding to and leading recovery from incidents (EPRR), to ensure NHS and partner organisations are joined up at times of greatest need, including taking on incident coordination responsibilities as delegated by NHS Englandand NHS Improvement.
- Functions NHS England and NHS Improvement will be delegating including commissioning of primary care and appropriate specialised services.
Duties (Section 19)
- 14Z32 Duty to promote NHS Constitution
- 14Z33 Duty as to effectiveness, efficiency etc
- 14Z34 Duty as to improvement in quality of services
- 14Z35 Duties as to reducing inequalities
- 14Z36 Duty to promote involvement of each patient
- 14Z37 Duty as to patient choice
- 14Z38 Duty to obtain appropriate advice
- 14Z39 Duty to promote innovation
- 14Z40 Duty in respect of research
- 14Z41 Duty to promote education and training
- 14Z42 Duty to promote integration
- 14Z43 Duty to have regard to wider effect of decisions
working with people
- Use public engagement and insight to inform decision–making
- Redesign models of care and tackle system priorities in partnership with staff, people who use care and support, and unpaid carers
- Work with Healthwatch and the voluntary, community, and social enterprise sector as key transformation partners
- Understand your community’s experience and aspirations for health and care
- Reach out to excluded groups, especially those affected by inequalities
- Provide clear and accessible public information about vision, plans, and progress to build understanding and trust
- Use community development approaches that empower people and communities, making connections to social action
Place Based Teams
The place leader on behalf of the Integrated Care Board, will work with place partners in an inclusive, transparent and collaborative way to contribute to:
- Strong and effective place-based partnerships between sectors with full involvement of all partners who contribute to the place’s health and care
- A continued strong strategic relationship with health and wellbeing boards.
They will have four main roles:
- to support and develop primary care networks (PCNs) which join up primary and community services across local neighbourhoods;
- to simplify, modernise and join up health and care (including through technology and by joining up primary and secondary care where appropriate);
- to understand and identify – using population health management techniques and other intelligence – people and families at risk of being left behind and to organise proactive support for them; and
- to coordinate the local contribution to health, social and economic development to prevent future risks to ill-health within different population groups.
They will need:
- appropriate resources, autonomy and decision-making capabilities to discharge these roles effectively.
- clear but flexible governance and accountability framework that enables collaboration around funding and financial accountability, commissioning and risk management, including the ability and mechanisms for delegated budgets.
- The ICB place-based team should be managed by a ICB Place Director or other named role.
- If delegation to Place is significant then there should be placed based senior management teams, led and line-managed by Place Directors, that will be responsible for all functions which are determined to be delegated to place level.
- The ICB place-based senior management team should have formal governance arrangements recognised and has congruence with the ICB/ICP and agreed mechanism of delegation. This management team and structure is separate from the ICP structure and the ICS executive.
- Place Director
- The place Director will manage the senior management team that delivers the place-based functions that are determined to be delegated to ICB (ICS) place-based teams. e.g. safeguarding, Infection Prevention and Control, learning disabilities, CHC, etc. Where performing a combined role they may also take on the duties set out below.
- ICP Director (or equivalent)
- Line managed by the Place Director, or reporting separately to the ICP, and will convene/lead the ICP and manage the transformation team and others that support the work and continued development of the ICP and PCNs.
- Place Planning and Transformation Lead
- Line managed by the Place Director, or reporting separately to the ICP, and will lead on planning and transformation including managing the place-based transformation team.
- Place Nurse/Quality Lead
- With professional oversight from the relevant ICS director but line managed by the Place Director.
- Place Finance Lead
- With professional oversight from the relevant ICS director but line managed by the Place Director.
- Place Director
- ICS Place-based teams should also be supported by the already established system wide HR and OD team. Corporate support should replicate this model.
- The ICPs should be supported by a team employed by the ICS, dedicated and based at place e.g. a CCG’s current transformation team. This may be managed separately e.g. by Place Planning and Transformation Lead/ICP Director, or similar, or fall within the remit of the Place Director (a matter for each Place to determine).
- The ICS place-based team would sit alongside any place-based provider collaborative and ICP and provide support and resource as appropriate to the ICP (e.g. BI, finance, admin support etc).